
Antibiotic Prescribing in Primary Healthcare Point Prevalence Survey (APC-PPS)
1.27 million deaths (95% UI 0·911–1·71 million) in 2019 were attributable to antibiotic resistant infections (ABR) with the highest burden in sub-Saharan Africa and South Asia. Improving appropriate antibiotic use is a key strategy in addressing antimicrobial resistance. Addressing inappropriate antibiotic use in many countries requires a balance between maintaining access to essential antibiotics and reducing inappropriate use of antibiotics; this requires understanding the clinical conditions, prescribing, access and us patterns.
The World Health Organisation (WHO) released the WHO Essential Medicines List (EML) AWaRe Antibiotic Book in November 2022, providing detailed guidance on the choice of antibiotic drug, dose and duration for 35 common infections in adults and children in primary healthcare and hospital settings. The AWaRe Antibiotic Book is built around the AWaRe framework (Access, Watch, Reserve), a classification for antibiotics related to their potential for selecting for resistance. The AWaRe Antibiotic Book recommends that almost 9 out of the 10 most common infections in primary healthcare should be treated with Access antibiotics. The book also highlights that low-risk patients with mild infections may not need antibiotic treatment.
The Antimicrobial Resistance, Prescribing, and Consumption Data to Inform Country Antibiotic Guidance and Local Action (ADILA) project is a Wellcome Trust funded study that aims to use clinical data together with data on antimicrobial consumption, resistance, and clinical outcomes to derive methods and tools to inform the development of national and local policies to improve antibiotic prescribing. One of the key objectives focuses on developing a methodological framework that, in the first instance, integrates clinical infection presentation/diagnoses with antibiotic prescribing from the primary healthcare setting.
Little data is available from the primary healthcare setting in LMICs describing the burden of clinical infections, aetiology of these diseases and antibiotic prescribing proportions for the infections. The available data are insufficient to analyse observed prescribing proportions for common infections, to inform national antibiotic prescribing policies and identify the potential of over, mis- or under-prescribing of antibiotics for specific conditions in many LMICs. This project aims to fill this gap and collect data linking the clinical indication with antibiotic prescribing in primary healthcare, based around the EML AWaRe categorisation and Antibiotic Book.
Project aims
This point prevalence survey aims to define the frequency of consultation for a variety of acute clinical presentations/diagnoses and the frequency and type of antibiotic prescribing for these infections in primary healthcare facilities. Specifically, we will:
- Quantify presentation rates of clinical infections of interest presenting to primary healthcare facilities
- Quantify the proportion of those presenting with clinical infections of interest that receive an antibiotic prescription (and those that do not)
- Of those who receive an antibiotic prescription, quantify the proportion of each antibiotic prescribed by AWaRe classification
The project also aims to explore the feasibility of using a tool such as this for surveillance of antibiotic use in the primary healthcare setting.
These results aim to inform models of observed and expected prescribing in primary healthcare as part of the wider ADILA project.
Study design
This study is a prospective, multi-centre, multi-country series of point prevalence surveys (PPS) conducted in a range of primary healthcare settings that prescribe / dispense antibiotics (e.g. primary care facilities, community health centres, hospital outpatients/ambulatory care, pharmacies, etc.) in at least 10 countries globally.
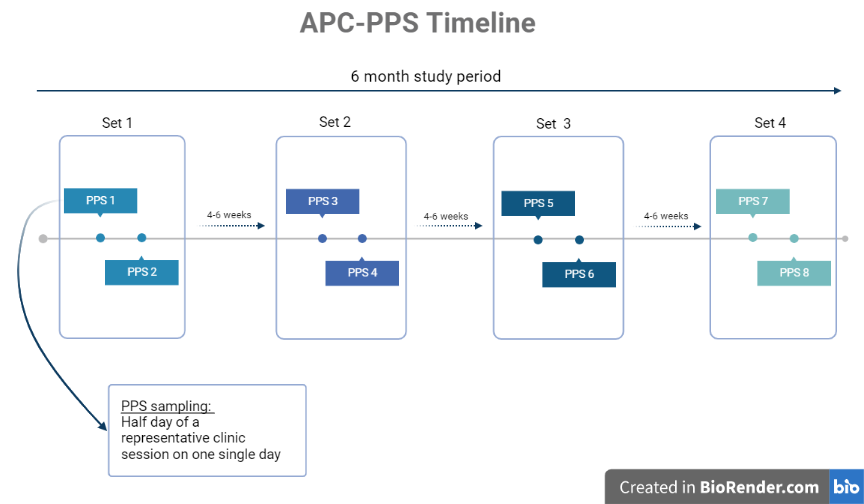
Study schedule
Sites will conduct 6-8 surveys over a 6-month period. Sites will conduct two surveys in a two week period and repeat this every 4-6 weeks for 6 months to provide an overview of the seasonal variability. We anticipate each survey will cover approximately 4 hours of a representative clinic session on a given day.
Eligibility
| Country | Facility/site | Patient |
|---|---|---|
| Any country will be eligible to participate in the point prevalence survey provided a country coordinator has been identified and trained and any national-level regulatory and ethical obligations are met. | Any facility within a country providing primary healthcare with clinical staff who can prescribe antibiotics are eligible to participate providing an ambassador is willing to lead the work. | All children and adults presenting with acute infection symptoms on the day of the survey should be included. Acute is defined as symptom(s) occurring for less than 2 weeks. |
Data collection
Data will be collected using a simple mobile app that allows for offline data collection. Data will be collected and managed using ODK (Open Data Kit, https://getodk.org/); data will be stored securely on a private Cloud-based server compliant with EU data protection laws and only available for analysis by the sponsoring organisation.
All data will be collected anonymously. There will be no identifiable information collected on patients and no information to link back to the patient.
Briefly, the following data will be collected:
| Age and sex | ||
|---|---|---|
| Relevant comorbidities (that may influence antibiotic prescribing decisions) | ||
| Infection symptoms of interest | Does the patient have / report having a fever? | • Fever >39°C • Persistent fever lasting 7 days or longer • Suspected enteric fever • Patient received anti-malarial prescription for this fever episode |
| Acute cough | • Cough >5 days • Shortness of breath/difficulty breathing • Chest pain |
|
| Sore throat/pharyngitis/tonsillitis | ||
| Facial pain or pressure/sinusitis | ||
| Runny nose/nasal congestion/coryza | ||
| Ear pain/acute otitis media | • Uni-lateral ear pain • Bi-lateral ear pain • Otorrhoea/ear discharge |
|
| Toothache/tooth abscess | ||
| Acute diarrhoea/gastroenteritis | • Bloody diarrhoea | |
| Increased urgency or frequency of urination/urinary tract infection (UTI) | • Blood in urine | |
| Painful urination | ||
| Genital discharge/sexually transmitted infection (STI) | ||
| Wound/burn/bite infection | ||
| Skin rash/spots – without swelling | ||
| Skin swelling/redness/warmth/pain | • Swollen lymph nodes | |
| Other primary presentation/diagnosis | • Please specify other symptoms/diagnosis: | |
| If antibiotics are prescribed/dispensed, which antibiotic, dose and duration of treatment will be recorded | ||
Proposed analyses
Data collected as part of this study will be analysed in the following way:
- Descriptive
- Rates of presentation for different clinical infections
- Prescribing proportion (to AWaRe categories)
- Modelling
- Clinical infection proportions – model expected antibiotic use at a national level
- Compare expected to observed national use (based on national guidelines)
- Surveillance framework
- Devise an ideal sampling framework for future surveillance studies
- To understand the optimal number of sites per country, number of patient encounters, frequency of sampling to reduce data bias
- To identify a core set of data variables – costs, feasibility and precision of different surveillance choices and the impact of losing each variable in the analysis
Data reporting and dissemination
Participating sites receive individual site-level summaries of the data presented by clinical infection, age groups and AWaRe categories after the study is complete. Dashboards for visualising results will be produced and code will be freely available for researchers to perform their own summary analysis (via GitHub).
Publication and dissemination of results from data collected through this policy will be guided by the principles of transparency and quality. The results from this study will be published in peer-reviewed journals, submitted as abstracts and presentations to conferences and presented as reports and policy documents. Analyses will be used to inform local policy decisions and discussed with the high-level global bodies (e.g. WHO). The investigators will be involved in developing and reviewing drafts of manuscripts, abstracts, reports, policy documents and other publications and presentations arising from the results of this project. All outputs using data from the project will be governed by the funder and project publication policy which includes acknowledgement of the project in all uses. Authorship for papers will be determined in accordance with the ICMJE guidelines and contributors will be acknowledged. Collaborators will also be supported in developing their own country-specific analyses, reports and publications. All analyses should be discussed and agreed with the Project Team prior to commencing.
Next steps
|
If you are interested in participating on this project, please reach out to Aislinn Cook at aicook@sgul.ac.uk and the ADILA team at apc_pps@sgul.ac.uk. Please identify if you would like to volunteer to be a coordinator for your country or as a participating site. You will be supported by the team at St. George’s University of London on training and to fulfil any necessary ethics and regulatory requirements to participate. |
Our partners
